

| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://www.jofem.org |
Original Article
Volume 12, Number 2, April 2022, pages 59-65

Sedentary Lifestyle Attenuates Positive Metabolic Effect of Regular Physical Exercise
Anna S. Isayevaa, b ![]() , Maryna M. Vovchenkoa
, Maryna M. Vovchenkoa ![]() , Olga V. Petyuninaa
, Olga V. Petyuninaa ![]()
aL.T. Malaya Therapy National Institute of the National Academy of Medical Sciences of Ukraine, Kharkiv 61139, Ukraine
bCorresponding Author: Anna S. Isayeva, Department of Chronic Non-Communicable Disease Prevention, GI “L.T. Malaya Therapy National Institute NAMSU”, Kharkiv 61039, Ukraine
Manuscript submitted February 11, 2022, accepted March 2, 2022, published online March 12, 2022
Short title: Negative Metabolic Effects of Sedentary Time
doi: https://doi.org/10.14740/jem797
| Abstract | ▴Top |
Background: The aim of the study was to evaluate the influence of the duration of sedentary time on blood lipids and anthropometric parameters in people practicing resistance training in leisure time.
Methods: Our study included 213 subjects without any history of cardiovascular disease. The target group (169 subjects) had at least two 90-min sessions of resistance training per week for at least 12 months prior to study commencing. The target group was divided into four groups according to their sitting time per week. There were no significant differences in physical activity between groups. The control group included 44 subjects without a history of cardiovascular diseases and without any regular physical activity. Anthropometric parameters, body composition, blood pressure, blood lipids and glucose levels were assessed. The International Questionnaire on long Physical Activity was used to assess physical activity and sedentary time. IBM® SPSS® Statistics 19 was used for statistical analysis.
Results: Patients were divided into four groups according to their sitting time. In the first group, the median of sitting time of 21.05 (14.00 - 21.25) h per week was spent seated; in the second group, 28.0 h (25.0 - 28.7); in the third group, 38.5 h (35.0 - 42.0) and in the fourth group, 56 h (49.0 - 56.7). After adjustment for age, sex and physical activity level, we observed a statistically significant association between sitting time and high-density lipoprotein cholesterol (HDL-cholesterol) and blood glucose levels. HDL-cholesterol progressively decreased with a prolonged sitting time (first group: 1.62 (1.45 - 1.75) mmol/L; fourth group: 1.31 (1.12 - 1.38) mmol/L) and blood glucose level increased (first group: 4.27 (3.90 - 4.63) mmol/L; fourth group: 4.63 (4.24 - 5.26) mmol/L).
Conclusions: Even in the subjects who are engaged in an appropriate time of resistance training, the total sitting time may exceed 56 h per week and attenuates positive effects of resistance training on HDL-cholesterol and blood glucose level.
Keywords: Physical activity; Sedentary time; Human anthropometric parameters; Blood lipids
| Introduction | ▴Top |
Sedentary lifestyle and low level of physical activity are the main modifiable risk factors of the cardiovascular diseases. Currently, the 2021 European Guidelines on cardiovascular disease prevention recommend at least 150 - 300 min of moderate intensity or 75 - 150 min of vigorous intensity aerobic physical activity a week, or an equivalent combination thereof, to reduce all-cause mortality, cardiovascular mortality, and morbidity [1]. In the Sport Medicine recommendations of 2020, 3.5 - 7.0 h of moderate or vigorous physical activity a week, or 30 - 60 min of a daily physical activity, are advised to deliver positive changes to the lipid profile. The active physical loads allow reducing the triglycerides level by 50%, increasing the cholesterol level of high-density lipoproteins (HDLs) by 5-10% and reducing the cholesterol level of low-density lipoproteins (LDLs) by 5%. Physical activity is also associated with other beneficial effects, such as an increased coronary artery flow and oxygen supply, and an increase in vessel diameter [2]. The transient myocardial ischemia induced by exercise increases tolerance to longer periods of ischemia experienced outside of the active period. Moreover, regular physical exercise decreases the levels of inflammatory markers [3] and platelet activation [4, 5]. The regular sporting activity positively influences levels of leptin, adiponectin and grehlin [6], optimizing eating behavior. Besides the positive influence on the cardiovascular system, regular physical exercises have positive effect on cognitive function [7, 8], mood [9], and reducing the risk of oncogenesis. However, despite the proven health benefits, patients often have very low compliance with recommendations to increase physical activity. Ironically, medical professionals frequently do not meet recommended physical activity levels themselves [10].
To overcome low compliance, a number of initiatives such as educational activities, providing monetary incentives, insurance coverage and others have been established around the globe. For example, in western countries, recreational and sport/fitness centers are one of the main sources of physical activity in working adults. At the same time, some research suggests that people who regularly visit sport centers 2 - 3 times a week, for 1 - 1.5 h duration, frequently also have a sedentary lifestyle outside these periods of activity. It has been shown that this kind of lifestyle is an independent factor, which negatively affects cardiovascular risk. According to Boyle et al, even the short-time physical activity limitation leads to the reduction of popliteal and brachial artery flow-mediated dilation and increased elevation of concentrations of endothelial microparticles. The negative changes in the bloodstream have already been observed on the fifth day after the physical activity limitation less than 5,000 steps a day [11]. The correlation of total and cardiovascular mortality with increased time spent in a sitting position has been demonstrated. The influence of sedentary lifestyle on blood lipid levels and its magnitude has not been investigated previously.
The aim of the study was to evaluate the influence of duration of sedentary time on blood lipids and anthropometric parameters in people practicing resistance training in leisure time. We hypothesized that people who have a predominantly sedentary lifestyle derive no strong beneficial effects from participating in leisure sports 2 - 3 times per week, as measured by metabolic and anthropometric parameters.
| Materials and Methods | ▴Top |
Participants
The study included people without any history of cardiovascular disease who have been practicing resistance training 2 - 3 times per week for at least 12 months prior to the inclusion in the study. “Resistance training” was defined as any exercise that causes the muscles to contract against an external resistance, which can be dumbbells, rubber exercise tubing, or any other object that causes the muscles to contract. All subjects had at least two sessions per week with a duration of about 90 min per session.
Exclusion criteria included involvement in the exercise regimens with a professional personal sport instructor or significant regular physical exercise other than resistance training; pregnancy; participation in weight reduction programs; significant diet restrictions such as plant-based diet, significant calorie restriction or other; any lipid lowering therapy; regular sport supplements intake; hemoglobin level below reference ranges; glomerular filtration rate below reference range.
Research design
Subjects (n = 268), which were included in the study, attended four different sport leisure centers in Kharkiv, Ukraine. Upon enrollment, we assessed the level of general physical activity with International Physical Activity Questionnaire (IPAQ), measured weight, height, waist and hip circumference and collected blood samples.
Subsequently, adults with a general physical activity below 25% (n = 52, IPAQ < 2,937) quartile and higher 75% quartile (n = 47, IPAQ > 4,194) were excluded from the analysis. The control group included 44 subjects without a history of cardiovascular disease who were not engaged in any regular physical activity. All participants were office workers and had similar socio-economic status.
Anthropometry
Weight, height, waist and hip circumference were assessed before eating in the morning in light clothing without any footwear. Body weight (to the nearest 0.1 kg) was measured using scales Technovagy (Ukraine, 2017). The body mass index (BMI) was calculated using the formula weight (kg)/height2 (m2). The proportion of muscular tissue and fat tissue, and the level of visceral fat were assessed using a bioelectrical impedance method (Composition Monitor BF511, Omron, China, 2015). Waist circumference between the lowest rib and the iliac crest when breathing normally was measured with a non-elastic tape. Two measurements of each anthropometric variable were performed, and the average was used for analysis. Blood pressure was measured according to the protocol recommended by the European Cardiology Society/Hypertension Society.
Biochemistry
Blood samples were taken from the cubital vein after nine fasting hours. Total cholesterol, triglycerides and HDL-cholesterol were evaluated with an enzymic method (kits: cholesterol liquicolor, HDL-cholesterol liquicolor, triglycerides liquicolor) using automatic biochemistry analyzer “HumaStar 200” (Human, Germany, 2005). Levels of LDL-cholesterol were calculated according to Friedewald W.T. formula. Blood glucose was assessed using the glucose oxidase method on a biochemical analyzer “Humalyzer 2000” (No. 18300-5397, kit: Glucose liquicolor).
Physical activity assessment
We used the IPAQ to assess physical activity and sedentary time. Data were analyzed using the IPAQ scoring protocol (https://sites.google.com/site/theipaq/scoring-protocol).
Statistical analysis
Continues variables were presented as median, 25% and 75% quartiles, and categorical variables were presented as absolute values and their percentages. Analysis of variance (ANOVA) test was used to compare age, anthropometric parameters, and lipids glucose, and uric acid levels. Multivariable linear regression model including age, sex and general physical activity, was used to adjust anthropometric parameters, blood lipids, glucose and uric acid values. P < 0.05 means the difference was statistically significant. IBM® SPSS® Statistics 19 was used for statistical analysis.
Ethical issues
The study protocol was approved by Ethics and Deontology Committee of L.T. Malaya National Institute of Therapy of National Academy of Medical Science of Ukraine (protocol No. 8; 08.06.2018). All procedures performed in the study were in accordance with the ethical standards of institutional, national research committee, and with the 1964 Helsinki Declaration and its later amendments.
| Results | ▴Top |
The target group was divided into four groups according to their sitting time per week. The median sitting time was 21.05 (14.00 - 21.25) h per week in the first group, 28.0 (25.0 - 28.7) h per week in the second group, 38.5 (35.0 - 42.0) h per week in the third group, and 56 (49.0 - 56.7) h per week in the fourth group. The level of general physical activity did not differ significantly between groups (Fig. 1). Sitting time in the control group was similar to the fourth group (55.4 (47.7 - 57.5) h per week), but the physical activity level was significantly lower.
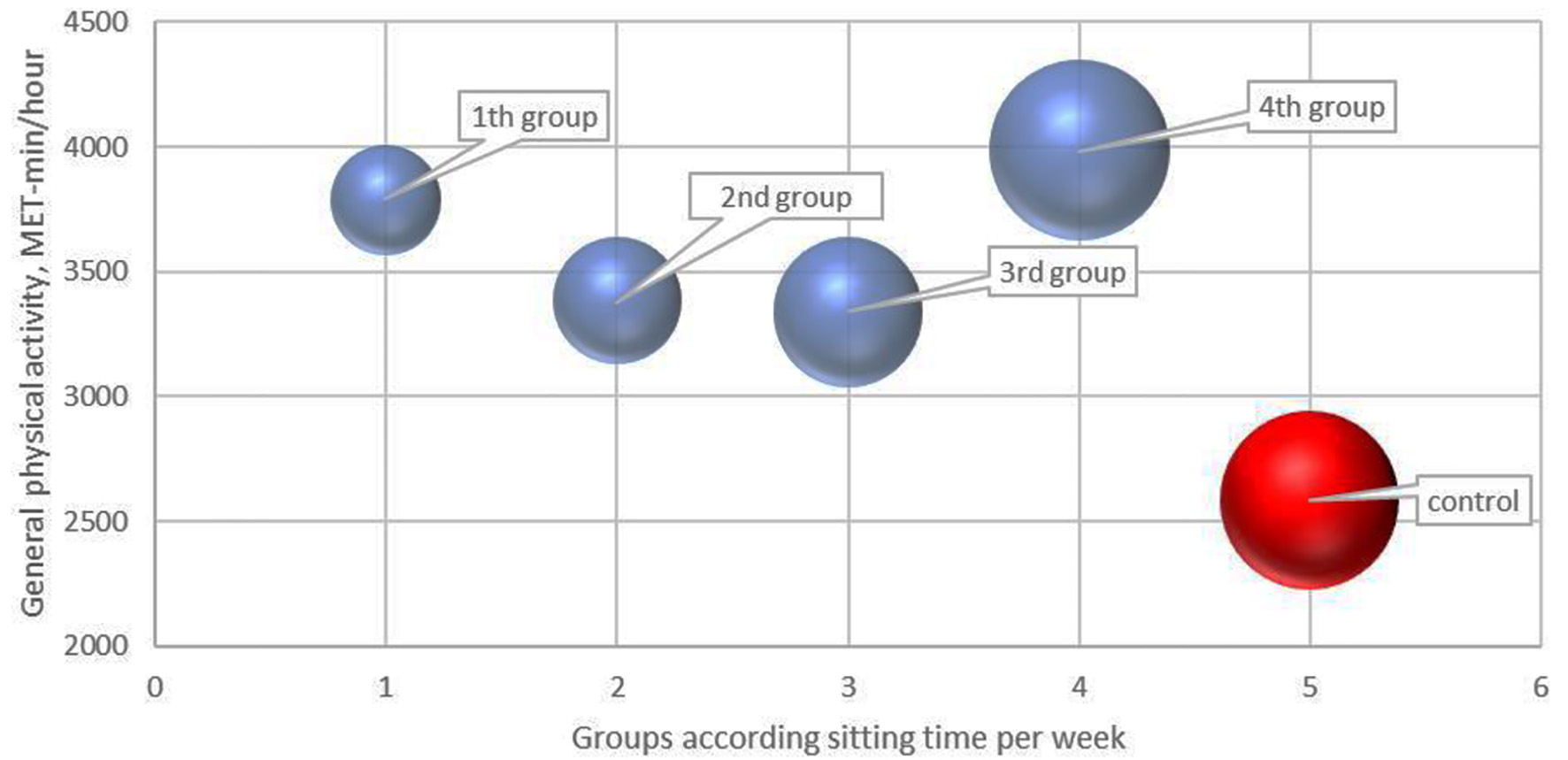 Click for large image | Figure 1. General physical activity levels and sitting time in the target and control groups. The size of the circle corresponds to sitting time in hours per week. |
Anthropometric parameters in four studied groups are presented in Table 1. Briefly, the age varied from 22 to 37 years old (median 23 - 31.5) and the proportion of female adults varied from 41.4% to 52.5%.
 Click to view | Table 1. Age, Sex and Anthropometric Parameters in Studied Population According to Sitting Time per Week in Groups |
After adjustment for age, sex, and physical activity, no statistically significant difference for anthropometric parameters was found. Although total cholesterol, LDL-cholesterol, triglycerides and uric acid levels did not differ significantly between groups, prolonged sitting time was associated with a lower HDL-cholesterol level and a higher blood glucose level (Table 2). HDL-cholesterol level progressively decreased from the first to fourth group time (first group: 1.62 (1.45 - 1.75) mmol/L; fourth group: 1.31 (1.12 - 1.38) mmol/L) and was the lowest in the fourth group (F = 4.67; P = 0.035) (Fig. 2). On contrary, blood glucose level increased with the prolonged sitting time (first group: 4.27 (3.90 - 4.63) mmol/L; fourth group: 4.63 (4.24 - 5.26) mmol/L) and was the highest in the fourth group (F = 17.6; P = 0.001).
Click to view | Table 2. Metabolic Parameters in Studied Population According to Sitting Time per Week in Groups |
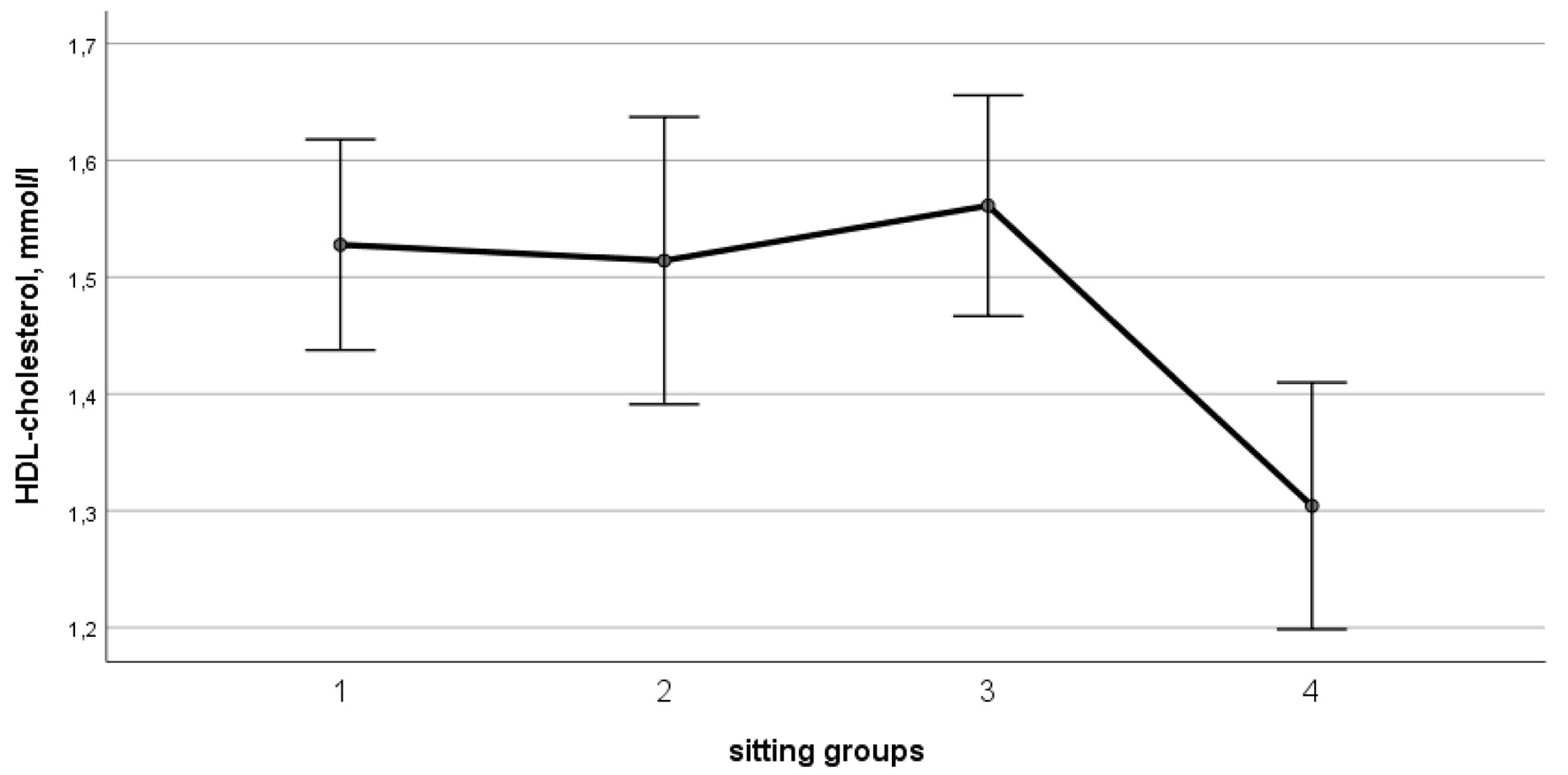 Click for large image | Figure 2. Age, sex and general physical activity-adjusted levels of HDL-cholesterol (F = 4.67; P = 0.035). HDL: high-density lipoprotein. |
| Discussion | ▴Top |
Variation in sitting time
We demonstrated that a decrease in HDL-cholesterol and an increase in blood glucose level (within reference ranges) were associated with a sedentary lifestyle, in spite of regular physical exercise. Our study complements the previous studies demonstrating that increasing the duration of physical activity does not necessarily protect from the negative effects of long sitting [12, 13]. It was suggested that sitting time was an independent risk factor for being overweight or obese and developing diabetes mellitus type 2, cardiovascular diseases and death.
However, in general, a high level of leisure-time physical activity is usually associated with less sitting time [14, 15]. Piirtola et al studied a Finnish twin cohort, which included more than 5,000 twin adults over 35 years. Investigators highlighted that aside from encouraging physical activity in leisure time, sitting time outside of those activities should be decreased as well [16]. This concept was supported by Paivarinne et al and Bonomi et al [17, 18].
A number of studies investigated the variation in sitting time in different groups. Matusiak-Wieczorek et al (2020) demonstrated that medical students generally participate in moderate-to-high intensity leisure sports yet sit for 5 to 8 h per day [19]. People with higher levels of education were reported to have a more sedentary lifestyle [20]. In the review of Mclaughlin et al (2020), the authors found that the individuals from higher-income countries tended to report sitting longer than those from lower-income countries, potentially on account of a higher proportion of the population being engaged in sedentary occupations, such as being employed in service-related industries, as opposed to agriculture or manufacturing [21]. Interestingly, the median of mean daily sitting time (by Tremblay et al [22] definition) was 4.7 h across all countries, corresponding to weekly sitting time in the first and second groups in our study. This highlights the fact that the participants in the fourth group and control group had significantly higher sitting time in comparison with the numbers previously reported for the general population.
Influence of sedentary lifestyle on cardiovascular outcomes, diabetes mellitus and mortality
In the meta-analysis by Bailey et al, which included the results of nine studies with a total of 448,285 participants, the total daily sitting time was associated with a significantly increased risk of cardiovascular disease (hazard ratio (HR): 1.29, 95% confidence interval (CI): 1.27 - 1.30, P < 0.001) and diabetes mellitus (HR: 1.13, 95% CI: 1.04 - 1.22, P < 0.001). Importantly, the risk of cardiovascular diseases and diabetes remained significant after adjustment for physical activity [23]. Similarly, a meta-analysis of 18 studies with 794,577 participants by Wilmot et al reported that higher levels of sedentary behavior were associated with a 112% increase in the risk of diabetes, 147% increase in the risk of cardiovascular disease, 90% increase in the risk of cardiovascular mortality and 49% increase in the risk of all-cause mortality [24]. Stamatakis et al in their study of 149,077 subjects over 8 years of follow-up also confirmed a negative effect of sitting on all-cause mortality. However, sitting was mostly associated with increased mortality only among the least physically active groups (sitting time more than 8 h per day) [20]. Reviews by Bakker et al (2018) and Henschel et al (2017) supported the claim that both increasing the level of physical activity and reducing the sitting time are important in preventing cardiovascular diseases [25, 26].
Influence of sedentary lifestyle on other metrics and measurements
Reid et al included data from 123 community-dwelling adults (65 - 84 years, 63% female). They demonstrated that a high total daily sitting time was independently associated with a lower proportion of lean mass and higher total body fat mass. More frequent breaks during the sitting period were associated with a 45% reduced risk of pre-sarcopenia. No associations with muscle strength or inflammation were found [27].
On contrary, in the study by Dempsey et al (2018), which included 3,429 participants at average age 58 ± 10 years without any history of diabetes or cardiovascular disease, blood lipids and adiposity indicators were significantly worse among higher levels of sitting for TV viewing and computer use. At the same time, occupational sitting after all adjustments did not negatively affect lipids and anthropometric parameters [28]. Similar findings were reported in adolescents. Penning et al reported that a reduction in school day sitting time resulted in significant improvements in apoB/apoA-1 ratio, with medium size effect on total cholesterol, HDL-cholesterol and total cholesterol/HDL ratio. An additional benefit of reducing sitting time was an improvement of cognitive function in a 6-month period [29]. Benatti and Ried-Larsen demonstrated that having breaks during a period of prolonged sitting has positive effect on metabolic outcomes [30]. Lurati also found an increased risk of trauma due to muscles weakness and detraining [31].
In our paper, we assessed metabolic parameters in young men and women without a history of cardiovascular events, who regularly attended sports centers for at least 12 months. Although they had similar levels of physical activity, sitting time varied significantly between groups. We demonstrated that it is not enough to have regular, time-limited physical exercises. Sitting more than 8 h per day attenuates the positive metabolic effects of strength exercises. It is therefore crucial to promote everyday active lifestyles, limit transport use where possible, give preference to stairs rather than elevators, and to take short periods of physical exercise during the working day.
Limitations
This study has several limitations. First, we studied adults attending major sport centers, which limits generalizability of the findings to the other social groups. While we enrolled adults with similar socio-economic status, the latter was not formally assessed. While we only enrolled patients with no cardiovascular disorders, family history was not assessed. Finally, a larger sample size would allow drawing more robust conclusions.
Conclusions
Even in the subjects who are engaged in an appropriate time of resistance training, the total sitting time may exceed 56 h per week and attenuates positive effects of resistance training on HDL-cholesterol and blood glucose level. Given our findings, additional educational activities may be promoted to ensure that adults maintain an appropriate level of physical activity every day. More research is needed to assess the influence of baseline sedentary lifestyle on cardiovascular outcomes.
Acknowledgments
Thanks to Olga Nazluyan and Daria Korystina for providing information about the study to sport centers attendants.
Financial Disclosure
This research received no external funding. This work was carried out under research program “Development of personalized programs of prevention of cardiovascular events in non-structured population” (#0119U001070) of L.T. Malaya National Institute of Therapy of National Academy of Medical Science of Ukraine.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Only participants who signed informed consent were included in the study.
Author Contributions
Anna S. Isayeva contributed to study design, data analysis, and literature review. Maryna M. Vovchenko and Olga V. Petyunina contributed to data collection and writing.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon request.
| References | ▴Top |
- Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Back M, Benetos A, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur J Prev Cardiol. 2022;29(1):5-115.
doi pubmed - Bruning RS, Sturek M. Benefits of exercise training on coronary blood flow in coronary artery disease patients. Prog Cardiovasc Dis. 2015;57(5):443-453.
doi pubmed - Suzuki K. Chronic inflammation as an immunological abnormality and effectiveness of exercise. Biomolecules. 2019;9(6):223.
doi pubmed - Heber S, Volf I. Effects of physical (In)activity on platelet function. Biomed Res Int. 2015;2015:165078.
doi pubmed - Lundberg Slingsby MH, Nyberg M, Egelund J, Mandrup CM, Frikke-Schmidt R, Kirkby NS, Hellsten Y. Aerobic exercise training lowers platelet reactivity and improves platelet sensitivity to prostacyclin in pre- and postmenopausal women. J Thromb Haemost. 2017;15(12):2419-2431.
doi pubmed - Dinas PC, Markati AS, Carrillo AE. Exercise-induced biological and psychological changes in overweight and obese individuals: a review of recent evidence. International Scholarly Research Notices. 2014;2014:1-11. https://doi.org/10.1155/2014/964627.
doi - Gaertner B, Buttery AK, Finger JD, Wolfsgruber S, Wagner M, Busch MA. Physical exercise and cognitive function across the life span: Results of a nationwide population-based study. J Sci Med Sport. 2018;21(5):489-494.
doi pubmed - Loprinzi PD, Frith E. Association between perceived physical activity and cognitive function in older adults. Psychol Rep. 2019;122(1):108-116.
doi pubmed - Johnson W, Mortensen EL, Kyvik KO. Gene-environment interplay between physical exercise and fitness and depression symptomatology. Behav Genet. 2020;50(5):346-362.
doi pubmed - Isayeva G, Vovchenko M, Reznik L, Isakova Y. Behavioral factors of cardiovascular risk in medical doctors of different specialties. Health Prim Car. 2017;1(3):1-3. https://doi.org/10.15761/HPC.1000113.
doi - Boyle LJ, Credeur DP, Jenkins NT, Padilla J, Leidy HJ, Thyfault JP, Fadel PJ. Impact of reduced daily physical activity on conduit artery flow-mediated dilation and circulating endothelial microparticles. J Appl Physiol (1985). 2013;115(10):1519-1525.
doi pubmed - Ekelund U, Steene-Johannessen J, Brown WJ, Fagerland MW, Owen N, Powell KE, Bauman A, et al. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet. 2016;388(10051):1302-1310.
doi - Patterson R, McNamara E, Tainio M, de Sa TH, Smith AD, Sharp SJ, Edwards P, et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. Eur J Epidemiol. 2018;33(9):811-829.
doi pubmed - Bauman A, Ainsworth BE, Sallis JF, Hagstromer M, Craig CL, Bull FC, Pratt M, et al. The descriptive epidemiology of sitting. A 20-country comparison using the International Physical Activity Questionnaire (IPAQ). Am J Prev Med. 2011;41(2):228-235.
doi pubmed - Bennie JA, Chau JY, van der Ploeg HP, Stamatakis E, Do A, Bauman A. The prevalence and correlates of sitting in European adults - a comparison of 32 Eurobarometer-participating countries. Int J Behav Nutr Phys Act. 2013;10:107.
doi pubmed - Piirtola M, Kaprio J, Svedberg P, Silventoinen K, Ropponen A. Associations of sitting time with leisure-time physical inactivity, education, and body mass index change. Scand J Med Sci Sports. 2020;30(2):322-331.
doi pubmed - Paivarinne V, Kautiainen H, Heinonen A, Kiviranta I. Relations between subdomains of physical activity, sedentary lifestyle, and quality of life in young adult men. Scand J Med Sci Sports. 2018;28(4):1389-1396.
doi pubmed - Bonomi AG, Plasqui G, Goris AH, Westerterp KR. Aspects of activity behavior as a determinant of the physical activity level. Scand J Med Sci Sports. 2012;22(1):139-145.
doi pubmed - Matusiak-Wieczorek E, Lipert A, Kochan E, Jegier A. The time spent sitting does not always mean a low level of physical activity. BMC Public Health. 2020;20(1):317.
doi pubmed - Stamatakis E, Gale J, Bauman A, Ekelund U, Hamer M, Ding D. Sitting Time, Physical Activity, and Risk of Mortality in Adults. J Am Coll Cardiol. 2019;73(16):2062-2072.
doi pubmed - McLaughlin M, Atkin AJ, Starr L, Hall A, Wolfenden L, Sutherland R, Wiggers J, et al. Worldwide surveillance of self-reported sitting time: a scoping review. Int J Behav Nutr Phys Act. 2020;17(1):111.
doi pubmed - Tremblay MS, Aubert S, Barnes JD, Saunders TJ, Carson V, Latimer-Cheung AE, Chastin SFM, et al. Sedentary Behavior Research Network (SBRN) - Terminology Consensus Project process and outcome. Int J Behav Nutr Phys Act. 2017;14(1):75.
doi pubmed - Bailey DP, Hewson DJ, Champion RB, Sayegh SM. Sitting Time and Risk of Cardiovascular Disease and Diabetes: A Systematic Review and Meta-Analysis. Am J Prev Med. 2019;57(3):408-416.
doi pubmed - Wilmot EG, Edwardson CL, Achana FA, Davies MJ, Gorely T, Gray LJ, Khunti K, et al. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: systematic review and meta-analysis. Diabetologia. 2012;55(11):2895-2905.
doi pubmed - Bakker EA, Sui X, Brellenthin AG, Lee DC. Physical activity and fitness for the prevention of hypertension. Curr Opin Cardiol. 2018;33(4):394-401.
doi pubmed - Henschel B, Gorczyca AM, Chomistek AK. Time Spent Sitting as an Independent Risk Factor for Cardiovascular Disease. Am J Lifestyle Med. 2020;14(2):204-215.
doi pubmed - Reid N, Healy GN, Gianoudis J, Formica M, Gardiner PA, Eakin EE, Nowson CA, et al. Association of sitting time and breaks in sitting with muscle mass, strength, function, and inflammation in community-dwelling older adults. Osteoporos Int. 2018;29(6):1341-1350.
doi pubmed - Dempsey PC, Hadgraft NT, Winkler EAH, Clark BK, Buman MP, Gardiner PA, Owen N, et al. Associations of context-specific sitting time with markers of cardiometabolic risk in Australian adults. Int J Behav Nutr Phys Act. 2018;15(1):114.
doi pubmed - Penning A, Okely AD, Trost SG, Salmon J, Cliff DP, Batterham M, Howard S, et al. Acute effects of reducing sitting time in adolescents: a randomized cross-over study. BMC Public Health. 2017;17(1):657.
doi pubmed - Benatti FB, Ried-Larsen M. The Effects of Breaking up Prolonged Sitting Time: A Review of Experimental Studies. Med Sci Sports Exerc. 2015;47(10):2053-2061.
doi pubmed - Lurati AR. Health Issues and Injury Risks Associated With Prolonged Sitting and Sedentary Lifestyles. Workplace Health Saf. 2018;66(6):285-290.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.