

| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website http://www.jofem.org |
Case Report
Volume 10, Number 2, April 2020, pages 54-56
Acute Pancreatitis in a Patient With Parathyroid Carcinoma: A Case Report
Rita Gervasia, Lucia Stella Curtob, c, Serena Fulginitib, Vincenzo Tiesib, Nadia Innaroa
aUnit of Endocrine Surgery, A.O.U. Mater Domini, Catanzaro, Italy
bUnit of Clinical Surgery, Department of Medical and Surgical Sciences, Magna Graecia University Medical School, Catanzaro, Italy
cCorresponding Author: Lucia Stella Curto, Unit of Clinical Surgery, Department of Medical and Surgical Sciences, Magna Graecia University Medical School, Catanzaro, Italy
Manuscript submitted February 25, 2020, accepted March 20, 2020
Short title: Acute Pancreatitis in Parathyroid Carcinoma
doi: https://doi.org/10.14740/jem636
| Abstract | ▴Top |
Parathyroid carcinoma is a rare endocrine malignancy. Clinical features of parathyroid carcinoma are mainly due to the effects of primary hyperparathyroidism (PHPT). Hypercalcemia produced by primary or secondary hyperparathyroidism is a rare and unclear cause of acute pancreatitis. Acute pancreatitis was rarely described before as the first manifestation of parathyroid carcinoma. The case concerns a 45-year-old man with hypercalcemia (15.9 mg/dL) and high levels of parathyroid hormone (1,089 pg/mL). Laboratory findings and ultrasound directed to right nodular goitre and an adenoma of the right lower parathyroid. The patient underwent right parathyroidectomy and ipsilateral loboistmectomy with laterocervical lymphadenectomy. On the first postoperative day he reported pain in the epigastrium, resistant to analgesics. Laboratory values and computed tomography (CT) scan, associated with clinical data, indicated exudative pancreatitis. It was treated with medical therapy; after some days there was resolution of symptoms and laboratory indexes returned to normal value. Histological examination diagnosed infiltrating parathyroid carcinoma that exceeded its capsule and infiltrated fibroadipose, muscular and perithyroidal tissues. After 18 months, no signs of local recurrence or metastases were observed. Our case report is unusual for its presentation. Acute pancreatitis can be observed in patient with PHPT, but it rarely reveals after parathyroidectomy. In patient who underwent parathyroidectomy with previous hypercalcemia associated with abdominal pain, acute pancreatitis should be suspected.
Keywords: Parathyroid carcinoma; Pancreatitis; Hypercalcemia; Parathyroid adenoma
| Introduction | ▴Top |
Parathyroid carcinoma is a rare endocrine malignancy with an annual incidence of < 1/1,000,000. It is difficult to diagnose this pathology preoperatively. The median patient age is 56 years [1, 2].
Clinical features of parathyroid carcinoma are mainly due to the effects of primary hyperparathyroidism (PHPT). Common presentations include signs and symptoms of hypercalcemia, bone disease, nephrolithiasis, nephrocalcinosis, osteopenia, pathological fractures, gastrointestinal disturbances, fatigue, and depression [3-5]. Parathyroid carcinoma is generally associated with an indolent and slowly progressive course. There are some clues that could suggest the presence of parathyroid carcinoma such as markedly elevated serum parathormone levels (usually more than five times of normal), severe hypercalcemia (usually > 14 mg/dL), a palpable neck mass and dysphonia.
Hypercalcemia due to primary or secondary hyperparathyroidism is a rare and unclear cause of acute pancreatitis although rarely it is the first manifestation. Mechanisms involved in its manifestation are not completely clear [6, 7]. There are very few studies that described acute pancreatitis as the first manifestation of parathyroid carcinoma; even less are those related to acute pancreatitis as early complication of a parathyroidectomy.
The first description of acute pancreatitis as a complication of parathyroidectomy was reported in 1950; literature report that pancreatitis can show from 1 h to 22 days after parathyroidectomy.
| Case Report | ▴Top |
A 45-year-old man with a resistant primitive hyperparathyroidism, hypercalcemia (15.9 mg/dL) and high parathormone level (1,089 pg/mL) was admitted to Endocrine Surgery Unit of A.O.U. Mater Domini of Catanzaro.
In his medical history he had chronic kidney failure, kidney stones, ankylosing spondylitis HLA-B27, hypertension, ulcerative colitis and right nodular goiter. He underwent surgical removal of giant cancer cells of the right femur. In 2015 and then in 2017, he was already subjected to right parathyroidectomy for adenoma but in another hospital. In December 2017, the ultrasound scan of the neck showed the presence of a hypoechoic lesion in the lower pole of the right thyroid lobe. In 2018 the patient was subjected to hexakis 2-methoxyisobutyl isonitrile (MIBI) scintigraphy showing a low probability scintigraphic picture for adenoma or hyperplasia of the parathyroid (Fig. 1). The neck computed tomography (CT) identified an elongated nodular formation in postero-inferior pole of the right lobe of the thyroid.
 Click for large image | Figure 1. Parathyroid scintigraphy. |
In June 2018, the patient was submitted to right parathyroidectomy and ipsilateral loboistmectomy with laterocervical lymphadenectomy. Postoperative course has been characterized, on the first postoperative day, from pain in the epigastrium, resistant to paracetamol. The blood tests (white blood cells 15.29 × 103/µL, neutrophils 90.3%, creatinine 2.49 mg/dL, amylase 1,393 U/L, lipase 1,189 U/L, calcium 11.9 mg/dL) and the abdomen CT suggested the diagnosis of exudative pancreatitis (Fig. 2). He was treated with medical therapy (intravenous water therapy, nasogastric tube, ranitidine), with resolution of symptoms and return to normal laboratory indexes. The abdomen CT scan was repeated after 24 h and it showed regression of peripancreatic edema. Complete regression of the edema was confirmed in CT scan performed after 1 month.
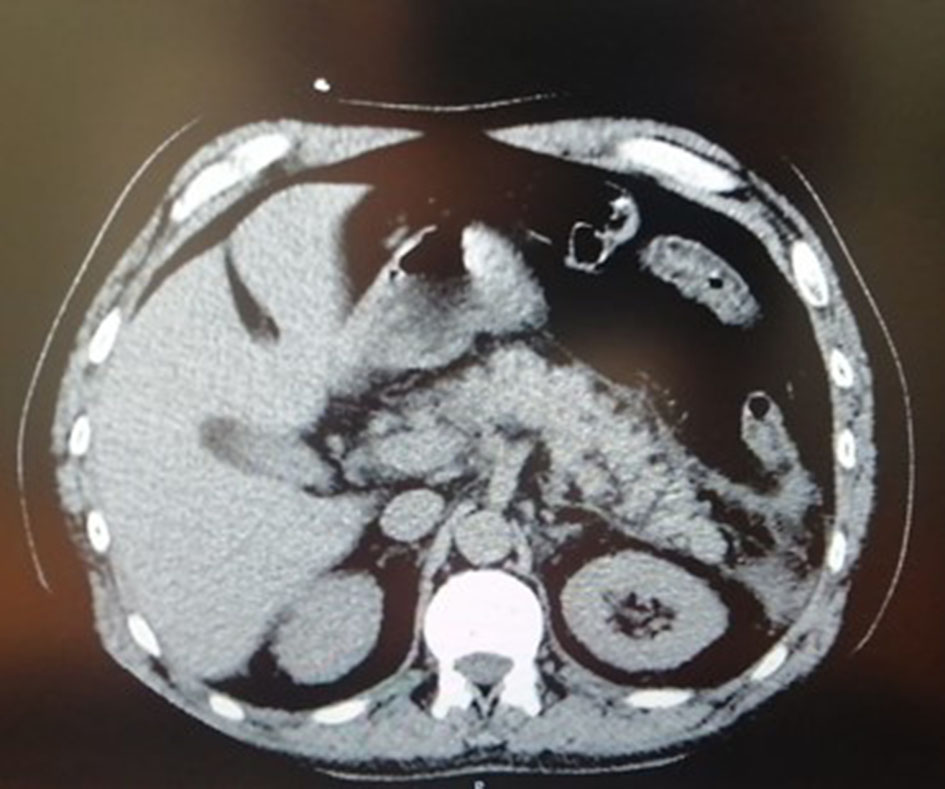 Click for large image | Figure 2. CT imaging of pancreatitis. CT: computed tomography. |
The histological examination of the parathyroid diagnosed infiltrating carcinoma that exceeded its capsule and infiltrated fibroadipose, muscular and perithyroidal tissues.
Actually, the patient is followed up and he is disease free.
| Discussion | ▴Top |
Typical clinical manifestations of parathyroid carcinoma are well known and they depend by high levels of parathyroid hormone and serum calcium; there are also unusual manifestations of hypercalcemia. Acute pancreatitis can reveal as manifestation of parathyroid adenoma or carcinoma, but, similarly, it can occur after parathyroidectomy. Acute pancreatitis after parathyroid excision is a rare complication; its incidence is about 0.2-9% [8]. Pathophysiological mechanisms that lead to pancreatitis are not completely clear and often opposed. Probably the rapid postoperative reduction of the serum calcium plays an important role. Preoperative serum calcium concentration above 12 mg/dL might cause pancreatic changes [6]. Another hypothesis is relative to manipulation of the gland during surgical neck exploration that causes an acute rinse of serum calcium that cannot be compensated by calcitonin. Moreover, microvascular clotting and thrombi formation could cause intraparenchymal activation of trypsinogen [6, 7].
Only few studies describe pancreatitis after parathyroidectomy [8, 9], while different studies described a hyperamylasemia post-parathyroidectomy without abdominal pain [10].
Our case report is unusual for its presentation; in literature there are very few cases of acute pancreatitis in patient with parathyroid carcinoma. Furthermore, right loboistmectomy was performed and it could be involved in pancreatitis genesis. In fact, there is a significant increase in pancreatitis incidence when thyroidectomy is performed at the same time as neck exploration for hyperparathyroidism (3% without thyroidectomy vs. 23%). It supports the protective role of calcitonin, because removal of part or all of the thyroid gland whose C-cells are responsible for the secretion of calcitonin acts to enhance the deficiency of calcitonin at the time of parathyroidectomy, thus increasing the incidence of pancreatitis [8].
The present case suggests relationship between acute pancreatitis and parathyroidectomy, even if the connection between these two entities remains questionable according to current literature.
Patients who refer abdominal pain after parathyroidectomy might have an associated pancreatitis, so suspicion should be maintained to warrant accurate and timely diagnosis.
Acknowledgments
None to declare.
Financial Disclosure
None to declare.
Conflict of Interest
None to declare.
Informed Consent
The patient has provided permission to publish these features of his case, and the identity of the patient has been protected.
Author Contributions
NI, RG and LSC contributed to think up the design of manuscript; VT and SF contributed to literature research and language revision. All authors wrote the manuscript.
Data Availability
The data described during the current study are available from the corresponding author on reasonable request.
| References | ▴Top |
- Weger AR, Lindholm JL. Discrimination of pancreatic adenocarcinomas from chronic pancreatitis by morphometric analysis. Pathol Res Pract. 1992;188(1-2):44-48.
doi - Lee PK, Jarosek SL, Virnig BA, Evasovich M, Tuttle TM. Trends in the incidence and treatment of parathyroid cancer in the United States. Cancer. 2007;109(9):1736-1741.
doi pubmed - Shane E. Clinical review 122: Parathyroid carcinoma. J Clin Endocrinol Metab. 2001;86(2):485-493.
doi pubmed - Otsuka Y, Kamata K, Minaga K, Takenaka M, Watanabe T, Kudo M. Acute pancreatitis with disturbed consciousness caused by hyperparathyroidism. Intern Med. 2018;57(21):3075-3078.
doi pubmed - Biondi A, Persiani R, Marchese M, Cananzi F, D'Ugo D. Acute pancreatitis associated with primary hyperparathyroidism. Updates Surg. 2011;63(2):135-138.
doi pubmed - Khoo TK, Vege SS, Abu-Lebdeh HS, Ryu E, Nadeem S, Wermers RA. Acute pancreatitis in primary hyperparathyroidism: a population-based study. J Clin Endocrinol Metab. 2009;94(6):2115-2118.
doi pubmed - Lenz JI, Jacobs JM, Op de Beeck B, Huyghe IA, Pelckmans PA, Moreels TG. Acute necrotizing pancreatitis as first manifestation of primary hyperparathyroidism. World J Gastroenterol. 2010;16(23):2959-2962.
doi pubmed - Reeve TS, Delbridge LW. Pancreatitis following parathyroid surgery. Ann Surg. 1982;195(2):158-162.
doi pubmed - Klepsch M, Bergenfelz A. Acute pancreatitis and amaurosis after right parathyroidectomy for primary hyperparathyroidism. Eur J Surg. 2000;166(4):336-339.
doi pubmed - Willems D, Hooghe L, Kinnaert P, Van Geertruyden J. [Postoperative pancreatitis, hyperamylasemia and amylase isoenzymes after parathyroidectomy for primary hyperparathyroidism]. Gastroenterol Clin Biol. 1988;12(4):347-353.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.