









| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website http://www.jofem.org |
Original Article
Volume 6, Number 6, December 2016, pages 178-182
Cigarette Smoking as a Relative Risk Factor for Metabolic Syndrome
Ihab I. Al-khalifaa, c, Shaimaa M. Mohammeda, Zahraa M. Alib
aFaculty of Pharmacy, Isra University, Amman, Jordan
bCollege of Pharmacy, University of Baghdad, Baghdad, Iraq
cCorresponding Author: Ihab Ibrahim Al-Khalifa, Faculty of Pharmacy, Isra University, Amman, Jordan
Manuscript accepted for publication December 12, 2016
Short title: Smoking for Metabolic Syndrome
doi: https://doi.org/10.14740/jem390e
| Abstract | ▴Top |
Background: Metabolic syndrome (MS) is a clustering of risk factors, such as central obesity, insulin resistance, diabetes, hypertension and atherosclerosis. Cigarette smoking is a strong risk factor for cardiovascular diseases; therefore, smoking may be considered as an important risk factor for MS. Smokers are at greater risk than non-smokers to become insulin-resistant and develop cardiovascular diseases. This study aimed to explore the association of cigarette smoking with MS and its components among Iraqi adults who were already smokers for more than 10 years.
Methods: This clinical study was conducted on 80 adult Iraqi subjects, aged 50 - 70 years. Subjects were divided into two groups according to their smoking status. Standard questionnaire was completed regarding smoking habits, medications, past medical history and physical activity. Blood pressure measurements and biochemical analysis involving fasting serum glucose and serum lipid profile (total cholesterol, high-density lipoprotein (HDL)-cholesterol and triglycerides (TG)) were done. The diagnosis of MS was based on the American Heart Association (AHA) and the National Heart, Lung, and Blood Institute (NHLBI) criteria.
Results: According to the AHA definition, this study showed that MS was higher in smokers than in non-smokers with the relative risk for MS. Furthermore, obesity and dyslipidemia were found to be in 65.6% and 80% of both study groups, respectively. Systolic (P = 0.026) and diastolic blood pressures (P = 0.03) were significantly higher in smokers compared with non-smokers. The present study clearly showed that total serum cholesterol, HDL-cholesterol and low-density lipoprotein (LDL)-cholesterol serum levels were higher in the smoker group; however, a statistical significance was not obtained. Serum TG level was significantly higher (P = 0.025) in smokers than in non-smokers. The remarkable increase in the prevalence of MS among the smokers and non-smokers was correlated with the involvement of more than one component of MS according to the AHA and NHLBI criteria.
Conclusions: The present study showed that tobacco smoke exposure increases the incidence of or worsens MS. Obesity and overweight give a comparable risk to smoking in adult subjects. Reducing the rate of cigarette smoking provides a beneficial effect on cardiovascular risk factors of this syndrome, such as body weight, blood pressure, blood cholesterol, and serum glucose.
Keywords: Metabolic syndrome; Cigarette smoking; Obesity
| Introduction | ▴Top |
Metabolic syndrome (MS) is a clustering of risk factors in a phenotypic clinical entity that increases the risk of heart disease and type2 diabetes [1], characterized by the presence of abdominal obesity, elevated blood pressure, high fasting glucose, atherogenic dyslipidemia and insulin resistance [2]. It is now established that components of MS are independently associated with cardiovascular disease (CVD) and type 2 diabetes, becoming targets of therapeutic changes in lifestyle, medications and surgery [3]. The American Heart Association (AHA) and the National Heart, Lung, and Blood Institute (NHLBI) recommend that MS could be identified as the presence of three or more of these components or metabolic risk factors that appear to directly promote the development of atherosclerotic CVD [4]. The prevalence of MS depends on age, gender and ethnic background, and increases with age from 6.7% in the age group of 20 - 29 years to 43.5% in the age group of 60 - 69 years [5]. Looking at various studies around the world, the prevalence varies from 7% in France, 24% in USA, 39.3% in Saudi Arabia to 45.5% and 46% in Tunisia and India, respectively [6]. The clinical management of MS may depend on lifestyle changes and minimizing the components that characterize the disorders mainly cigarette smoking, the incidence of tobacco exposure such as cigarette smoking is exceptionally high in these countries, in which cigarette smoking is the single most important preventable cause of death and illness [6]. The pathogenesis of both MS and the multi-organ damage from chronic tobacco exposure and smoking has been more or less well documented [2]. Individuals who smoke experience a wide range of CVD, insulin resistance, elevated catecholamine levels which contribute to an elevated heart rate and blood pressure, and hypercholerterolemia [7]; thus smokers demonstrate many features that are similar to MS. These similarities indicated that smoking might be related to increased risk of the MS. The association of these independent factors, and the mechanism by which it influences each other needs to be elucidated further, as both pose grate threat to public health [6, 7]. This study aimed to determine whether parts of the adverse effect of smoking are contributing factors for the presence of MS in adults who were already smokers for more than 10 years.
| Materials and Methods | ▴Top |
This clinical study was conducted on adult Iraqi volunteers and approved by the scientific and ethic committee for clinical research there. All participants were informed of the nature of the screening and all were subjected to standard questionnaire comprising smoking habits, medications, past medical history, physical activity, and blood pressure. Eighty males and females aged 50 - 70 years participated in the study and were divided into two groups according to their smoking status. Group A (smokers) included 40 smokers with a mean age (± standard deviation (SD)) of 53.5 ± -4.19 years, and age range of 50 - 63 years, who were heavily smokers for more than 10 years at past. Group B (non-smokers) included 40 non-smokers with a mean (± SD) age of 56.85 ± 6.49 years, and age range of 50 - 70 years, who were apparently healthy and never smoked at past.
Written informed consent was obtained from each participant. A checklist including age, sex, smoking, amount of smoking, blood pressure, weight, height, body mass index (BMI), and waist circumference was obtained from each participant. Blood pressure was measured by a standard sphygmomanometer after 15 min rest in a sitting position. Blood pressure was measured twice with at least 30 min intervals and the mean of two blood pressure measurements was considered as participant’s blood pressure. Waist circumference was measured at the midpoint between the lowest rib and the upper border of the right iliac crest, while body weight and height were taken from each subject nearest to each 0.1 cm. MS was defined based on the AHA/NHLBI criteria. According to this definition, participants with three or more of the following five criteria had MS: 1) abdominal obesity determined by elevated waist circumference (≥ 102 cm in men and ≥ 88 cm in women); 2) elevated triglycerides (TG) (≥ 150 mg/dL); 3) reduced high-density lipoprotein (HDL)-cholesterol (< 40 mg/dL in men and < 50 mg/dL in women); 4) elevated blood pressure (systolic blood pressure (SBP) ≥ 130 mm Hg or diastolic blood pressure (DBP) ≥ 85 mm Hg); and 5) elevated fasting glucose (≥ 100 mg/dL). For each subject, the following biochemical test was done based on blood samples taken in the morning after 12 h of fasting. TG, fasting serum glucose (FSG), serum cholesterol and HDL were measured using an enzymatic colorimetric method with readymade kits: glucose kit (Biomaghreb Company), TG kit (Biomaghrab company), HDL kit (Biomaghrab company) and cholesterol kit (Biomaghrab company), while estimation of serum low-density lipoprotein (LDL) was obtained from Friedwald equation: LDL (mg/dL) = total cholesterol - (HDL + TG/5).
Statistical analysis
Data were expressed as mean ± SD and analyzed by SPSS20 software. P < 0.05 was considered as statistically significant. Frequencies were presented as valid percentage; paired t test was used for comparison among groups. Relative risk factors such as obesity, dyslipidemia and hypertension for the development of MS among smoker and non-smoker groups were calculated as a ratio of the probability of an event occurring in the exposed group versus a non-exposed group.
| Results | ▴Top |
This study was conducted on 40 smokers with a mean (± SD) age of 53.5 ± 4.19 years, and age range of 50 - 63 years and 40 non-smokers with a mean (± SD) age of 56.85 ± 6.49 years and age range of 50 - 70 years. According to the AHA definition, this study showed that MS was noted in 55% of the smokers and 45% of the non-smokers. Obesity and dyslipidemia were found to be 65.6% and 80% in both groups, respectively, and hypertension was found to be higher among smokers. Table 1 highlights the descriptive characteristics of smokers and non-smokers and revealed that there was no significant difference between the two groups in respect to their age, waist circumference, and BMI. SBP and DBP were significantly higher in smoker group (P = 0.026 and P = 0.03, respectively). Table 2 demonstrated that total cholesterol, HDL-cholesterol and LDL serum levels were higher in smoker group; however, statistical significance was not obtained. Serum TG level was significantly higher in smokers than in non-smokers (P = 0.025). Serum glucose level showed impaired glucose tolerance in both groups. As shown in Table 3, the relative risk for MS was found to be 1.22 by smoking; furthermore, other conventional risk factors for obesity, dyslipidemia and hypertension were shown to be 1.44, 2.5 and 1.75 among smokers, while for non-smokers were shown to be 4.31, 1.42 and 0.45, respectively. The distribution of MS components among the smokers and non-smokers is presented in Figure 1 as defined by the AHA and NHLBI criteria.
 Click to view | Table 1. Descriptive Characteristics of Smokers and Non-Smokers |
Click to view | Table 2. Biochemical Parameters Among Smokers and Non-Smokers Groups |
Click to view | Table 3. Relative Risk for Various Metabolic Syndrome Factors Among Smokers and Non-Smokers Groups |
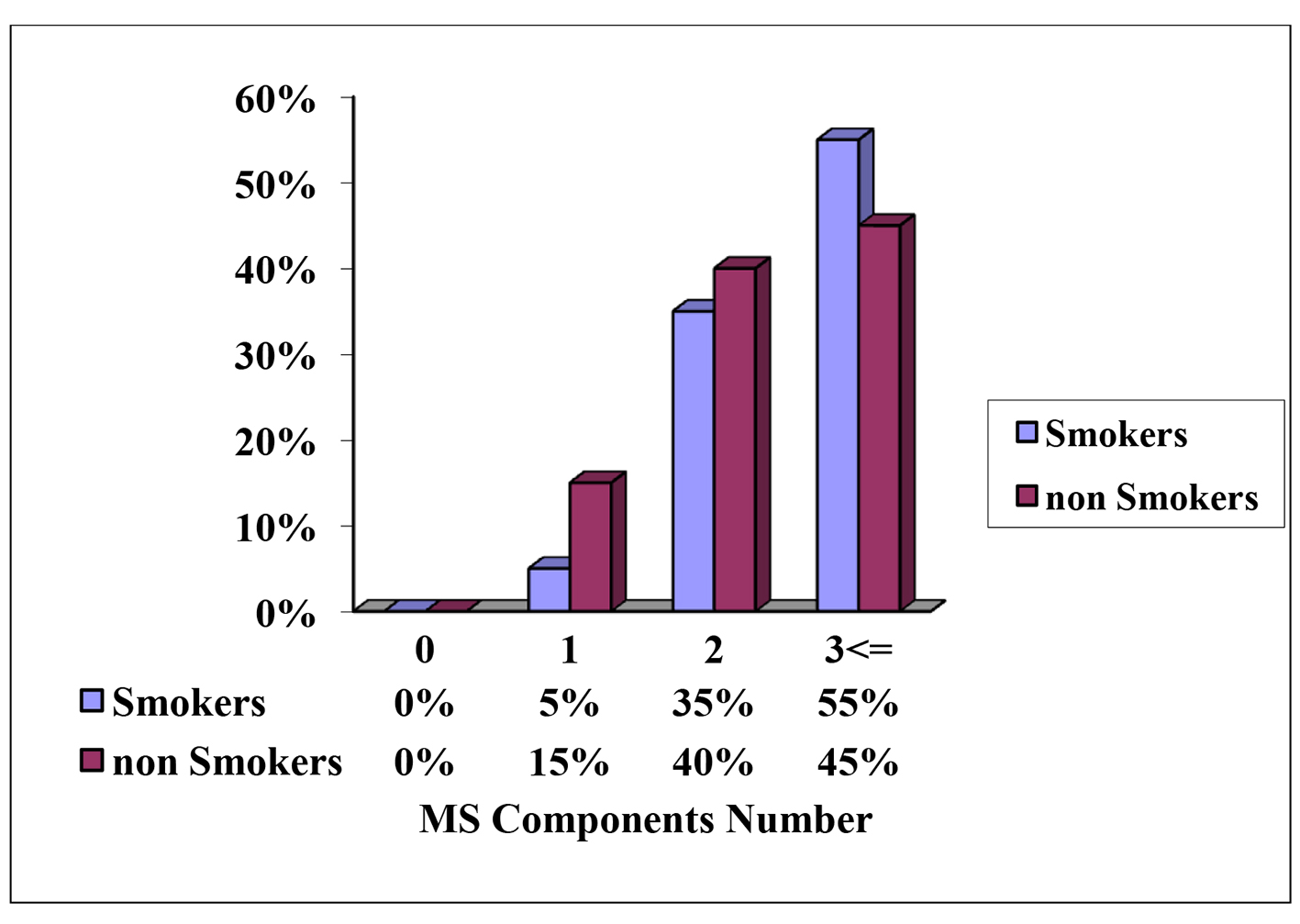 Click for large image | Figure 1. Distribution of the smokers and non-smokers according to the components of metabolic syndrome according to the American Heart Association (AHA) and the National Heart, Lung, and Blood Institute (NHLBI) in valid percentage. |
| Discussion | ▴Top |
MS is a combination of unfavorable health factors including abdominal obesity, dyslipidemia, hypertension and glucose intolerance [4], and is strongly associated with increased risk of CVD and type 2 diabetes [8]. Smoking has also been implicated as a risk factor for MS. Earlier studies have suggested that overall tobacco use is associated with an increased risk of MS [9, 10], most likely due to its effects on waist circumference, blood lipids and blood pressure [11, 12].
This study demonstrated that the associated risk for developing MS among smokers was 1.22, which was in accordance with other studies that demonstrate smoking as risk factor for developing of MS [13, 14]. On the other hand, obesity relative risk was about 4.31 for developing MS in non-smokers as compared to 1.44 among smokers.
A growing body of evidences indicates that tobacco smoke is independently associated with insulin resistance and that the insulin resistance and tobacco smoke are clearly associated with dyslipidemias [13]. Smokers also demonstrate many features that are similar to MS, and these similarities indicate that smoking might increase the risk of MS [15, 16]. This theory is supported by some scientific studies which were conducted in middle-aged adults who are more likely to develop MS [13, 17]. Some studies among teenagers who were at high risk for being overweight and were also exposed to smoke also reveal a higher risk for developing MS [15, 18]. Other conditions associated with MS include physical inactivity, aging, excess body fat and genetic predisposition which may be a risk factor for developing of MS [19, 20].
Smoking affects the metabolic rate in that the decrease in metabolic rate is usually higher in the smokers due to nicotine suppression, which in turn decreases the release of serotonin and nor adrenaline hormones, giving the concept that smokers have lower anthropometric indexes than non-smokers [21]. Results from previous studies show that increase in smoking can contribute to abdominal obesity, consistent with our finding [22]. SBP and DBP were higher in the smokers which highlight the effects of smoking status in arterial stiffness, and considered as a strong predictor of smoking-related vascular disease [23]. Smoking itself affects lipid metabolism partly by its contribution to central adiposity and insulin resistance, which can alter the lipid and lipoprotein profile by interfering with fat metabolism [23, 24]. Furthermore, cigarette particulate matter alters catecholamine release which in turn affects VLDL and LDL concentration to favor their accumulation in the blood ending in lower HDL level and promoting atherogenesis [17]. Dyslipidemia relative risk for developing MS was 2.5% among smokers in our study and TG level was significantly higher in smoking group as compared with the non-smokers. This came in accordance with previous studies which showed statistically significant alterations in the levels of lipoproteins and TG [25, 26]. As presented in this study, the association of smoking with insulin resistance and impaired glucose tolerance was reported in many studies previously [3, 27].
Conclusion
From this study, one can conclude that tobacco smoke exposure increases the incidence of MS occurrence and worsens the effect of MS; however, it is not the only risk factor. Obesity and overweight give a comparable risk for MS development in Iraqi adults.
| References | ▴Top |
- Chandola T, Brunner E, Marmot M. Chronic stress at work and the metabolic syndrome: prospective study. BMJ. 2006;332(7540):521-525.
doi pubmed - Buckland G, Salas-Salvado J, Roure E, Bullo M, Serra-Majem L. Sociodemographic risk factors associated with metabolic syndrome in a Mediterranean population. Public Health Nutr. 2008;11(12):1372-1378.
doi pubmed - Vidigal Fde C, Ribeiro AQ, Babio N, Salas-Salvado J, Bressan J. Prevalence of metabolic syndrome and pre-metabolic syndrome in health professionals: LATINMETS Brazil study. Diabetol Metab Syndr. 2015;7:6.
doi pubmed - Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735-2752.
doi pubmed - Ogbera AO. Prevalence and gender distribution of the metabolic syndrome. Diabetol Metab Syndr. 2010;2:1.
doi pubmed - Haddad FH, Mahafza SM. Impact of metabolic syndrome's components on the development of cardiovascular disease in a Jordanian cohort with metabolic syndrome. Saudi Med J. 2008;29(9):1299-1305.
pubmed - Chelland Campbell S, Moffatt RJ, Stamford BA. Smoking and smoking cessation -- the relationship between cardiovascular disease and lipoprotein metabolism: a review. Atherosclerosis. 2008;201(2):225-235.
doi pubmed - Slagter SN, van Vliet-Ostaptchouk JV, Vonk JM, Boezen HM, Dullaart RP, Kobold AC, Feskens EJ, et al. Associations between smoking, components of metabolic syndrome and lipoprotein particle size. BMC Med. 2013;11:195.
doi pubmed - Nakanishi N, Takatorige T, Suzuki K. Cigarette smoking and the risk of the metabolic syndrome in middle-aged Japanese male office workers. Ind Health. 2005;43(2):295-301.
doi pubmed - Sun K, Liu J, Ning G. Active smoking and risk of metabolic syndrome: a meta-analysis of prospective studies. PLoS One. 2012;7(10):e47791.
doi pubmed - Chiolero A, Faeh D, Paccaud F, Cornuz J. Consequences of smoking for body weight, body fat distribution, and insulin resistance. Am J Clin Nutr. 2008;87(4):801-809.
pubmed - Chen CC, Li TC, Chang PC, Liu CS, Lin WY, Wu MT, Li CI, et al. Association among cigarette smoking, metabolic syndrome, and its individual components: the metabolic syndrome study in Taiwan. Metabolism. 2008;57(4):544-548.
doi pubmed - Jamshidi L, Seif A, Vazinigheysar H. Comparison of Indicators of Metabolic Syndrome in Iranian Smokers. Zahedan J Res Med Sci. 2014;16(1):55-58.
- Kim BJ, Kim BS, Sung KC, Kang JH, Lee MH, Park JR. Association of smoking status, weight change, and incident metabolic syndrome in men: a 3-year follow-up study. Diabetes Care. 2009;32(7):1314-1316.
doi pubmed - Miyatake N, Wada J, Kawasaki Y, Nishii K, Makino H, Numata T. Relationship between metabolic syndrome and cigarette smoking in the Japanese population. Intern Med. 2006;45(18):1039-1043.
doi pubmed - Calo WA, Ortiz AP, Suarez E, Guzman M, Perez CM. Association of cigarette smoking and metabolic syndrome in a Puerto Rican adult population. J Immigr Minor Health. 2013;15(4):810-816.
doi pubmed - Li S, Yun M, Fernandez C, Xu J, Srinivasan SR, Chen W, Berenson GS. Cigarette smoking exacerbates the adverse effects of age and metabolic syndrome on subclinical atherosclerosis: the Bogalusa Heart Study. PLoS One. 2014;9(5):e96368.
doi pubmed - Weitzman M, Cook S, Auinger P, Florin TA, Daniels S, Nguyen M, Winickoff JP. Tobacco smoke exposure is associated with the metabolic syndrome in adolescents. Circulation. 2005;112(6):862-869.
doi pubmed - Kaur J. Assessment and Screening of the Risk Factors in Metabolic Syndrome. Med Sci. 2014;2:140-152.
doi - Filozof C, Fernandez Pinilla MC, Fernandez-Cruz A. Smoking cessation and weight gain. Obes Rev. 2004;5(2):95-103.
doi pubmed - Nerin I, Beamonte A, Gargallo P, Jimenez-Muro A, Marqueta A. [Weight gain and anxiety levels in recent ex-smokers]. Arch Bronconeumol. 2007;43(1):9-15.
doi - Saarni SE, Pietilainen K, Kantonen S, Rissanen A, Kaprio J. Association of smoking in adolescence with abdominal obesity in adulthood: a follow-up study of 5 birth cohorts of Finnish twins. Am J Public Health. 2009;99(2):348-354.
doi pubmed - Jatoi NA, Jerrard-Dunne P, Feely J, Mahmud A. Impact of smoking and smoking cessation on arterial stiffness and aortic wave reflection in hypertension. Hypertension. 2007;49(5):981-985.
doi pubmed - Kong C, Nimmo L, Elatrozy T, Anyaoku V, Hughes C, Robinson S, Richmond W, et al. Smoking is associated with increased hepatic lipase activity, insulin resistance, dyslipidaemia and early atherosclerosis in Type 2 diabetes. Atherosclerosis. 2001;156(2):373-378.
doi - Nakashita Y, Nakamura M, Kitamura A, Kiyama M, Ishikawa Y, Mikami H. Relationships of cigarette smoking and alcohol consumption to metabolic syndrome in Japanese men. J Epidemiol. 2010;20(5):391-397.
doi pubmed - Berlin I, Lin S, Lima JA, Bertoni AG. Smoking Status and Metabolic Syndrome in the Multi-Ethnic Study of Atherosclerosis. A cross-sectional study. Tob Induc Dis. 2012;10(1):9.
doi pubmed - Oh SW, Yoon YS, Lee ES, Kim WK, Park C, Lee S, Jeong EK, et al. Association between cigarette smoking and metabolic syndrome: the Korea National Health and Nutrition Examination Survey. Diabetes Care. 2005;28(8):2064-2066.
doi
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.