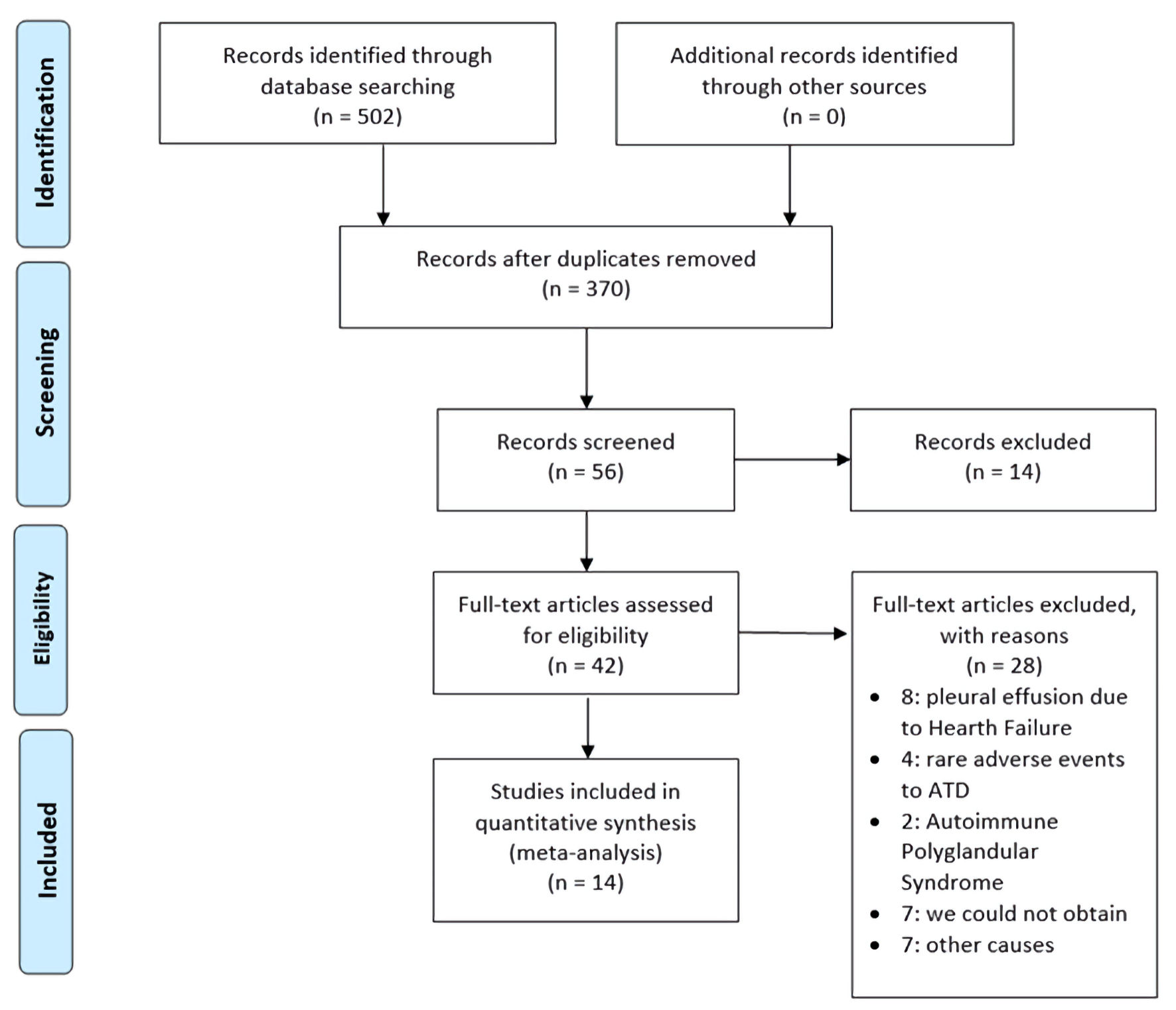
Figure 1. Flow diagram of screening and selection of articles adapted from the PRISMA. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; ATD: antithyroid drug.
| Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc |
| Journal website https://www.jofem.org |
Review
Volume 12, Number 1, February 2022, pages 1-9
Pleuropericardial Compromise Associated With Graves’ Disease: A Systematic Review
Figure
Tables
| Reference | Age/sex | Immunological signs | Cardiac tamponade | Serosa | Characteristics of the effusion | Effusion’s management (diagnosis, biopsy, drainage) | GD treatment | Additional treatment | Follow-up | Outcomes | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pericardial | Pleural | Pharmacological | RAI | T | |||||||||
| M: male; F: female; GD: Graves’ disease; NS: does not specify; NR: does not refer; -: does not apply; Pe: pericarditis; Pl: pleurisy; RAI: radioiodine therapy. | |||||||||||||
| Airel et al, 2013 [39] | 24/M | Bilateral orbitopathy, lid lag | No | Pe | NR | NR | - | Atenolol, methimazole | Yes | NR | Prednisone | 3 months | Hypothyroidism, mild regression of orbitopathy |
| Bui et al, 2016 [43] | 76/M | No | Yes | NR | Hematic, exudate | Left-sided, transudate | Pericardiocentesis, thoracentesis | Methimazole | NR | NR | Heparin, corticoids, aspirin, diltiazem | 5 months | Asymptomatic |
| Clarke et al, 2002 [44] | 35/F | Lid lag | Yes | Pe | Yes/NS | Yes, bilateral/NS | Pericardiocentesis | Carbimazole, propranolol | Yes | NR | NR | 18 months | Euthyroid, no effusions |
| Clarke et al, 2002 [44] | 47/F | NR | No | Pe | Yes/NS | NR | NR | Propranolol, carbimazole | NR | NR | Heparin | 12 months | Asymptomatic |
| Cullen et al, 2017 [45] | 17/M | Bilateral orbitopathy, lid lag | No | Pe | No | NR | - | Methimazole, propranolol | NR | NR | Lorazepam | 1 month | No recurrence, proptosis persisted |
| Gondal et al, 2020 [46] | 24/M | Thyroid enlargement | No | Pe | Yes/NS | NR | NR | Carbimazole, propranolol | NR | NR | Ibuprofen, omeprazole | 3 months | Euthyroid, clinically and biochemically |
| Gupta et al, 2015 [47] | 40/M | NR | No | Pe | NR | NR | - | Propylthiouracil, labetolol | NR | NR | Ibuprofen | 10 days | Follow-up was recommended |
| Hosseini et al, 2019 [48] | 69/F | NR | Yes | NR | Exudate | Left-sided/NS | Pericardiocentesis | NR | NR | NR | Paracetamol | 4 weeks | Pericardial effusion (re-hospitalized) |
| Inami et al, 2014 [49] | 69/F | NR | No | Pe | No | NR | - | Methimazole, β antagonist | NR | NR | Ibuprofen, colchicine | 4 weeks | Euthyroid state |
| Khalid et al, 2011 [7] | 68/F | NR | No | Pe, Pl | Yes/NS | Yes/exudate | Pleural biopsy | Carbimazole, propranolol | NR | NR | NR | 6 months | Euthyroid state |
| Koo et al, 2012 [50] | 42/M | NR | No | Pe | Yes/NS | NR | NR | Methimazole | NR | NR | Ibuprofen, colchicine | 3 months | No recurrence |
| Kortekaas et al, 2014 [51] | 44/M | No | NR | Pe | NR | NR | Dash | Thiamazole, metoprolol | NR | NR | Carbasalate calcium, colchicine | Outpatient follow-up was scheduled | |
| Nakata et al, 2005 [40] | 43/M | NR | No | No | Hematic, exudate | NR | Pericardiocentesis | Methimazole, iodine (drug) | NR | NR | NR | 1 month | No recurrence |
| Rodriguez et al, 2006 [41] | 68/M | No | No | Pl | NR | Yes, right-sided/exudate | Diagnostic thoracentesis, pleural biopsy | NR | Yes | NR | NR | 12 months | Asymptomatic |
| Teague et al, 2009 [42] | 42/F | Edema | Yes | Pe | Hematic, exudate | Yes/NS | Pericardiocentesis | Carbimazole and propranolol | NR | NR | Diuretics | NS | “She remained well” |
| Reference | Diagnosis of PPC | ||
|---|---|---|---|
| Clinical symptoms | Imaging compatible with PPC | ECG compatible with pericarditis | |
| Pe: pericarditis; ECG: electrocardiogram; CT: computed tomography; ECO: echocardiography; MRI: magnetic resonance imaging; Pe-Ef: Pericardial effusion; Pl-Ef: Pleural effusion; NR: does not refer. | |||
| Airel et al, 2013 [39] | Pe: substernal, pleuritic chest pain relieved in the upright position | NR | PR segment depression, and diffuse ST segment elevation |
| Bui et al, 2016 [43] | NR | ECO: Pe-Ef; chest X-ray: Pl-Ef | NR |
| Clarke et al, 2002 [44] | NR | NR | NR |
| Clarke et al, 2002 [44] | NR | ECO: Pe-Ef | NR |
| Cullen et al, 2017 [45] | Pe: pain improved sitting upright and leaning forward | NR | Diffuse ST-segment elevation |
| Gondal et al, 2020 [46] | Pe: sharp chest pain, increased by breathing, improved by leaning forward | ECO: small global pericardial effusion | Diffuse ST elevation and PR depression in limb leads |
| Gupta et al, 2015 [47] | Substernal, pleuritic chest pain; improved on leaning forward; mild dyspnea; friction rub | ECO: Pe-Ef | PR depressions and downsloping TP-segments, except in leads aVR and V1 |
| Hosseini et al, 2019 [48] | Cardiac tamponade: jugular vein distension, pulses paradoxes, and muffled heart sounds | ECO: Pe-Ef; chest X-ray: Pl-Ef | NR |
| Inami et al, 2014 [49] | Retrosternal chest pain which increased with deep breathing and position change | ECO: normal; CT: thickened pericardium | Diffuse ST-segment elevation in all leads except aVR and V1. |
| Khalid et al, 2011 [7] | Loud pericardial rub and raised jugular venous pressure | ECO: Pe-Ef; chest X-ray: Pl-Ef | NR |
| Koo et al, 2012 [50] | Pain increased with deep breathing and position change | ECO: Pe-Ef; MRI: thickened pericardium and Pe-Ef | Diffuse concave ST-segment elevation in all leads except aVR and V1 |
| Kortekaas et al, 2014 [51] | Sharp retrosternal pain; precordial friction rub chest pain | ECO: no Pe-Ef | Concave ST-segment elevation in all leads except aVR and aVL |
| Nakata et al, 2005 [40] | Does not refer symptoms of pericarditis | ECO; chest X-ray; CT: Pe-Ef | NR |
| Rodriguez et al, 2006 [41] | Pl-Ef | Chest X-ray and CT (Pl-Ef) | Atrial fibrillation |
| Teague et al, 2009 [42] | Pl-Ef | ECO: Pe-Ef; chest X-ray: Pl-Ef | Does not refer |
| Study | Selection | Ascertainment | Causality | Reporting | Total score | ||
|---|---|---|---|---|---|---|---|
| a. Does the patient(s) represent(s) the whole experience of the investigator (center) or is the selection method unclear to the extent that other patients with similar presentation may not have been reported? | b. Was the exposure adequately ascertained? | c. Was the outcome adequately ascertained? | d. Were other alternative causes that may explain the observation ruled out? | e. Was follow-up long enough for prognosis outcomes to occur? | f. Is the case described with sufficient details to allow other investigators to replicate the research or to allow practitioners make inferences related to their own practice? | ||
| Airel et al, 2013 [39] | Yes | Yes | Yes | No | No | Yes | 4 |
| Bui et al, 2016 [43] | Yes | Yes | Yes | Yes | No | Yes | 5 |
| Clarke et al, 2002 [44] | No | Yes | Yes | Yes | Yes | No | 4 |
| Clarke et al, 2002 [44] | No | Yes | Yes | Yes | Yes | No | 4 |
| Cullen et al, 2017 [45] | No | Yes | Yes | No | No | Yes | 3 |
| Gondal et al, 2020 [46] | No | Yes | Yes | Yes | No | Yes | 4 |
| Gupta et al, 2015 [47] | Yes | Yes | No | No | No | Yes | 3 |
| Hosseini et al, 2019 [48] | Yes | Yes | Yes | Yes | No | Yes | 5 |
| Inami et al, 2014 [49] | No | Yes | Yes | Yes | No | Yes | 4 |
| Khalid et al, 2011 [7] | No | Yes | Yes | Yes | Yes | Yes | 5 |
| Koo et al, 2012 [50] | Yes | Yes | Yes | Yes | No | Yes | 5 |
| Kortekaas et al, 2014 [51] | No | Yes | No | Yes | No | Yes | 3 |
| Nakata et al, 2005 [40] | No | Yes | Yes | Yes | No | Yes | 4 |
| Rodriguez et al, 2006 [41] | Yes | Yes | Yes | Yes | Yes | Yes | 6 |
| Teague et al, 2009 [42] | Yes | Yes | No | No | No | Yes | 3 |