
Figure 1. Abdominal ultrasound: enlarged pancreas with diffuse calcifications suggestive of chronic pancreatitis. There is a bulky aneurysmatic vascular lesion with a mural thrombus, located in the superior aspect of the pancreatic tail that seems to stem from the splenic artery.
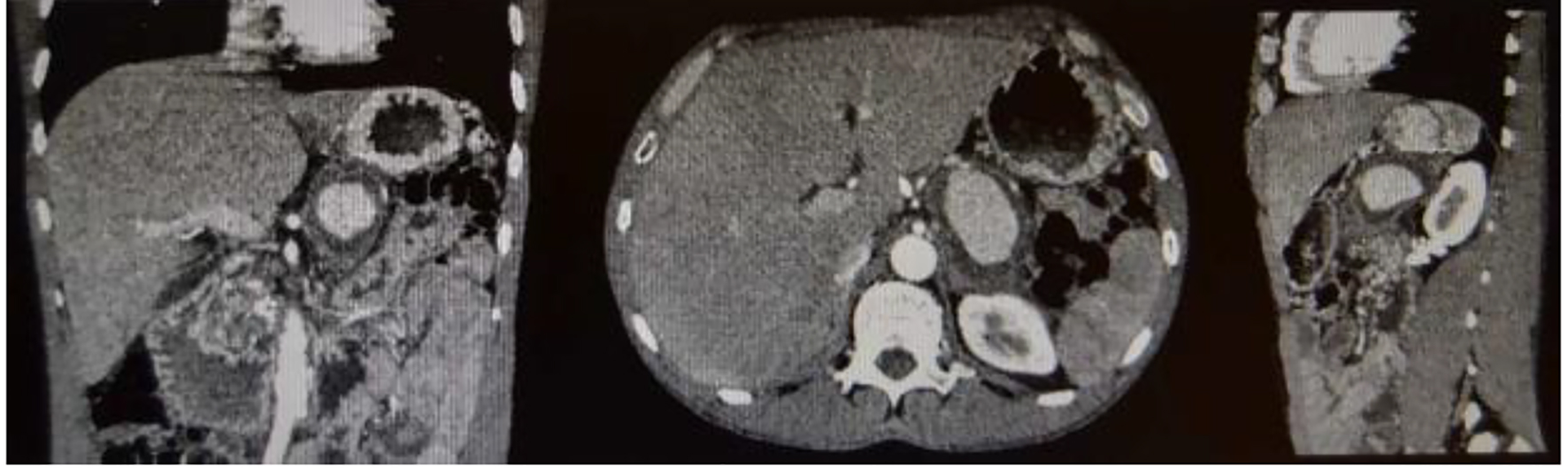
Figure 2. Contrast-enhanced abdominal CT scan. There is an evident aneurysmal vascular lesion with at least 68 mm of longer axis, exhibiting a mural thrombus, closely related with the splenic artery, which is located antero-superiorly. It enhances less intensely in the dominant arterial phase compared to the branches of the celiac trunk. Its probable starting point is the splenic artery, given its topography and clinical context. The Doppler color coding with YingYang signal also indicates that it is an arterial structure.