*Average article statistics from the last 12 months data
COVID-19 RESEARCH
The COVID-19 outbreak presents the unprecedented challenge for world public and medical practitioners and health care providers, the post COVID-19 condition (or long COVID) includes long term symptoms which may persist for months or years after SARS-CoV-2 infection. We will consider submissions related to all aspects of COVID-19 and Long COVID, and process the manuscripts in priority.
Journal of Endocrinology and Metabolism, ISSN 1923-2861 print, 1923-287X online, Open Access
Article copyright, the authors; Journal compilation copyright, J Endocrinol Metab and Elmer Press Inc
Journal website http://www.jofem.org
Letter to the Editor
Volume 7, Number 3, June 2017, pages 98-99
Construction of Effective and Safe Glycemic Control in the Elderly by Using Continuous Glucose Monitoring
Koki Kakutaa, b, Hiroki Adachia, b, Hidekatsu Yanaia, c
aDepartment of Internal Medicine, National Center for Global Health and Medicine Kohnodai Hospital, Chiba, Japan bThese authors equally contributed to this work. cCorresponding Author: Hidekatsu Yanai, Department of Internal Medicine, National Center for Global Health and Medicine Kohnodai Hospital, 1-7-1 Kohnodai, Ichikawa, Chiba 272-0034, Japan
Manuscript submitted May 16, 2017, accepted May 30, 2017 Short title: Letter to the Editor doi: https://doi.org/10.14740/jem425w
Severe hypoglycemia is significantly associated with increased risks of a range of adverse clinical outcomes [1]. An increased risk for developing dementia by older patients with diabetes who have had episode of severe hypoglycemia has been suggested [2]. Further, patients with dementia and diabetes appear to be at greater risk for severe hypoglycemia [2]. However, excellent evidence on glycemic control in the elderly is lacking, and optimal treatment needs to be constructed collaboratively with patients, incorporating the likelihood of benefits and harms and patients preferences about treatment in older adults with type 2 diabetes [3].
To show the usefulness of continuous glucose monitoring (CGM) to determine safe and effective glycemic control in the elderly, we present our old patient who showed asymptomatic severe hypoglycemia during sleeping. An 83-year-old type 2 diabetic female patient (body height, 151.4 cm; body weight, 56.7 kg; BMI, 24.7 kg/m2) was admitted to our hospital due to poor glycemic control. She has been treated by ingestion of alogliptin (25 mg) before breakfast, and repaglinide (1.0 mg) before every meal, and injection of insulin glargine U300 (10 U) before breakfast. On admission, her plasma glucose and HbA1c level were 334 mg/dL and 8.7%, respectively.
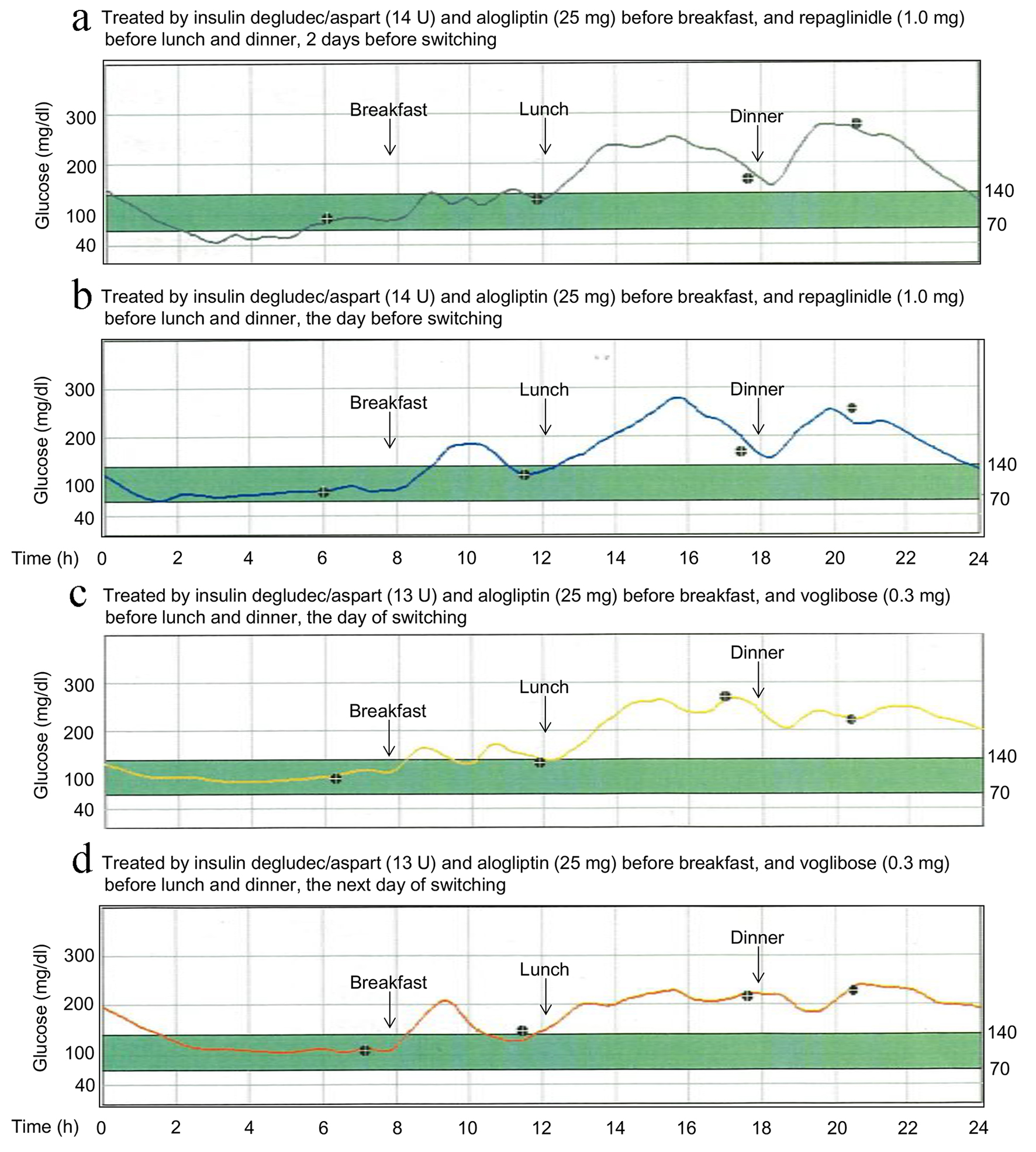
We changed insulin treatment from insulin glargine U300 (10 U) to insulin degludec (IDeg)/insulin aspart (IAsp) (14 U) which is a soluble conformation of two distinct insulin analogues in the ratio of 70% ultra-long-acting IDeg and 30% rapid-acting IAsp [4]. We stopped ingestion of repaglinide before breakfast because of the addition of IAsp before breakfast. We also switched from repaglinide (1.0 mg before lunch and dinner) to α-glucosidase inhibitor (α-GI), voglibose (0.3 mg before lunch and dinner).
We present the result of CGM which showed the effect of switching from repaglinide to voglibose on glycemic control in Figure 1. CGM showed hypoglycemia early at morning (from 2 to 6 o’clock in the morning) (Fig. 1a, b) during the treatment using repaglinide. After the switching to voglibose, hypoglycemia early at morning was disappeared (Fig. 1c, d). In addition, maximal glucose level and amplitude of glucose excursion decreased, in spite of reduction of insulin dose (Fig. 1d).
Figure 1. Continuous glucose monitoring showing the effect of switching from repaglinide to voglibose for the treatment for type 2 diabetes in old women.
Repaglinide is a short-acting, insulin-releasing agent, and has been suggested to lessen the risk of long-lasting hypoglycemia [5], however, which was observed in our patient. We should consider the development of severe hypoglycemia in the elderly whose drug clearance is diminished when we use glinides. Furthermore, our observation indicated that α-GI does not induce long-lasting hypoglycemia and also ameliorates glycemic control in combination with insulin as compared with glinides.
We think that benefits and harms about treatment for diabetes depend largely on individuals, and individual differences get larger by aging. Therefore, we strongly recommend the construction of safe and effective glycemic control in the elderly by using CGM.
Conflicts of Interest
The authors declare that they have no conflicts of interest concerning this article.
Zoungas S, Patel A, Chalmers J, de Galan BE, Li Q, Billot L, Woodward M, et al. Severe hypoglycemia and risks of vascular events and death. N Engl J Med. 2010;363(15):1410-1418. doipubmed
Meneilly GS, Tessier DM. Diabetes, Dementia and Hypoglycemia. Can J Diabetes. 2016;40(1):73-76. doipubmed
Lipska KJ, Krumholz H, Soones T, Lee SJ. Polypharmacy in the Aging Patient: A Review of Glycemic Control in Older Adults With Type 2 Diabetes. JAMA. 2016;315(10):1034-1045. doipubmed
Ma Z, Parkner T, Christiansen JS, Laursen T. IDegAsp: a novel soluble insulin analogs combination. Expert Opin Biol Ther. 2012;12(11):1533-1540. doipubmed
Guay DR. Repaglinide, a novel, short-acting hypoglycemic agent for type 2 diabetes mellitus. Pharmacotherapy. 1998;18(6):1195-1204. pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Endocrinology and Metabolism is published by Elmer Press Inc.